Dr Julia Martins
Dr Julia Martins 
According to the United Nations (UNFPA-UNICEF), there are 4.2 million girls around the world at risk of being subjected to female genital mutilation/cutting (FGM/C) in 2022. FGM consists of cutting or removing the external female genitals, and it is often performed without anaesthesia by untrained people, resulting in life-long physical and emotional problems for the person who undergoes it. FGM is a human rights violation and ending it is a deeply feminist fight.
FGM can vary (there are four kinds of FGM), and is performed today in more than thirty countries (and that’s not including the United States or Europe). Still, whenever I read news about FGM, I am struck by how little its history is discussed, or how it is similar to many other bodily interventions, from medieval to Victorian times. This is a millenary practice, stretching from ancient Egypt to the present, and spreading through many parts of the globe. Yet the term ‘female genital mutilation’ is itself a Western concept; many people from performing cultures prefer the term ‘female circumcision’.
It is telling that it is the Western nomenclature that is most often used in the discourse about FGM: the term ‘mutilation’ conjures up violence and even barbarism, something we do not want to associate with ourselves. There’s an inherent ‘otherness’ when FGM is discussed in developed countries, as though it were a practice relegated to the ‘global South’, stuck in misogynistic traditions and unable to fully embrace modernity. The way that the media portray FGM often makes us associate it with people fundamentally different from us, living in far away places. Yet that could not be farther from the truth. As always, things are a little bit more complicated than that.
Bodies that do not conform to socio-cultural expectations (be they religious, sexual, or medical) have long been subject to interventions. Unruly bodies could be ‘corrected’ by surgery, for instance, or ‘purified’ through religious ceremonies. I wrote recently about how non-binary bodies could be threatening to how medieval and early modern people understood the world. It was not uncommon for these intersex bodies to be ‘corrected’ through surgery. The same could be said for female bodies with ‘excessively large’ genitalia, which should also be ‘corrected’ surgically.
The Persian physician
Two centuries later, when these texts were translated into Latin, they started to be studied by Western physicians. By the 14th century, European surgeons cited
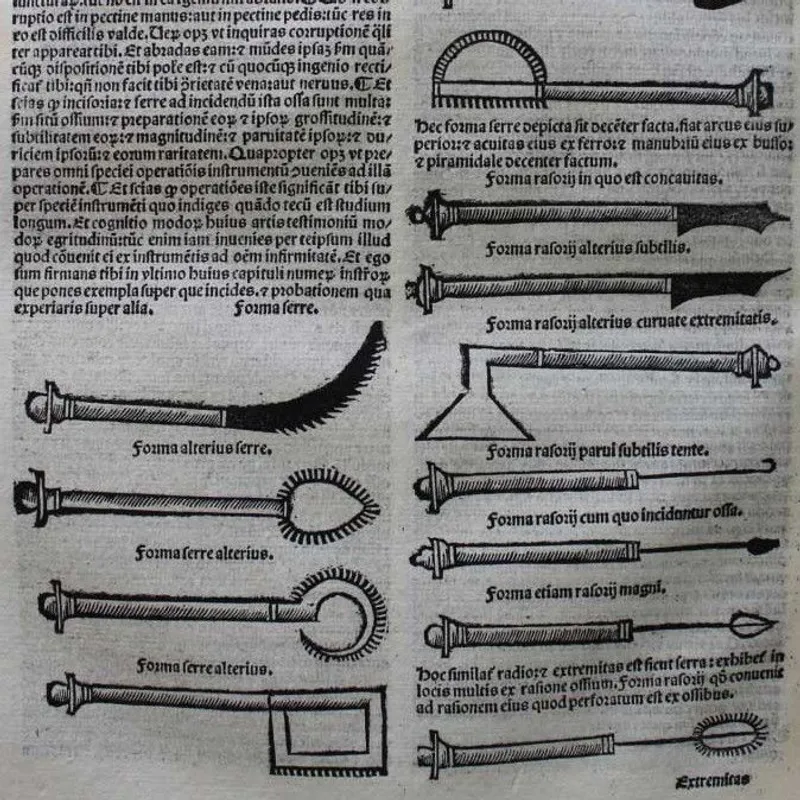

These ‘corrective’ surgeries were never commonplace in medieval times, whether in the Middle East or in Western Europe. They may have been occasionally performed, but their main importance lies in how often they were discussed by medical practitioners. Similarly, clitoridectomy was recommended (and indeed practised for a short period) during
However, clitoridectomies were still performed in the United States to ‘treat’ masturbating girls and women in the same period – and they continued until the 1960s. It was also recommended to ‘help’ women orgasm during penetrative sex. These surgeries were considered valid medical practices yet are rarely discussed today.
It might seem counter-intuitive to compare FGM to surgical interventions in different social, geographical, and temporal contexts. But the clitoris and its symbolic role as the site of female sexuality are central in the examples cited here. Whether performed by specialised medical practitioners or by laypeople, all these ‘corrections’ and ‘treatments’ on female bodies derived from their specific cultural contexts. Medieval ‘hermaphrodites’ might display enlarged clitorises that could threaten binaries and gender roles, while 19th-century perceptions of masturbation as pathological could mean it had to be prevented. Controlling (and dominating) the female body and women’s sexuality is the thread connecting these seemingly disparate activities.
FGM as we know it today has a long history and encompasses many different practices that vary from a geographic, ethnic, and cultural perspective. Furthermore, it was not always the same throughout the centuries in which it was (and is) performed. My goal here is not to generalise, but to continue to learn more about FGM today and how we can help in the fight to eradicate it and protect women and girls. However, we should be careful not to distance ourselves too sharply from performing communities. Medical practitioners have performed forms of FGM, especially clitoridectomy, in Europe and in the United States, until not too long ago. It is not a ‘non-Western’ practice. It’s not someone else’s problem. FGM is a human rights issue that concerns all of us, especially feminists.

* This text was written in collaboration with the wonderful people from The Vavengers. You can support this incredible charity here.
References
Albucasis, Cyrurgia Albucasis cum cauterijs et alijs instrumentis (Venice, 1500).
Avicenna, Liber Canonis Avicenne (Venice, 1507).
Isaac Baker Brown, On Surgical Diseases of Women (London, 1861).
Guy de Chauliac,
Further Reading
Leah DeVun, The Shape of Sex (New York, 2021).
Sarah Rodriguez, Female Circumcision and Clitoridectomy in the United States (New York, 2018).