Dr Julia Martins
Dr Julia Martins 
Imagine this: It’s 1910, and you’re strolling through an international medical conference in Europe. The legacies of Louis Pasteur and Robert Koch are being celebrated for discovering that tiny microbes—not “bad air”—cause diseases. Revolutionary! Groundbreaking! The audience applauds these European geniuses who saved humanity!
And then, from the back of the room, a Brazilian doctor stands up: “Excuse me, but while you were identifying bacteria in your fancy European labs, my colleagues and I have been eradicating yellow fever by hunting mosquitoes, discovering entirely new tropical diseases, and vaccinating entire cities. Also, a Cuban doctor named Finlay figured out mosquito transmission TWENTY YEARS before Walter Reed’s ‘discovery,’ and you all laughed at him.”
Awkward silence
Ok, this never happened. But it could have! The history of germ theory we’re usually taught is like a family photo with the European scientists front and center while their Latin American colleagues are barely visible in the background. Today, we’re adjusting the focus to reveal the full picture—and trust me, the overlooked parts are fascinating.
Miasmas, Mosquitoes, and Misconceptions
Let’s start with a quick history refresher. Until the late 19th century, most doctors worldwide believed that many diseases came from “miasmas” – poisonous vapors rising from swamps, sewage, and decomposing matter. Got cholera? Probably those bad smells from the river. Yellow fever? Must be those foul vapors from the port. This “miasma theory” dominated medicine for a long time.
Then, in the 1860s, Louis Pasteur in France demonstrated that microorganisms caused fermentation and putrefaction, not spontaneous generation. Shortly after, Robert Koch in Germany developed rigorous methods to isolate specific bacteria, identifying the causes of anthrax (1876), tuberculosis (1882), and cholera (1884). Together, they established what we now call “germ theory” – the radical idea that invisible microorganisms, not bad air, cause specific diseases. European medical journals celebrated this paradigm shift as if science began and ended in Paris and Berlin. But here’s where our story takes an interesting turn – because while Europeans were just beginning to grasp the basics of microbes, physicians in the tropics were already making remarkable leaps forward.


In 1881, a Cuban physician named
And you know what happened? He might as well have been talking to a brick wall. The scientific community collectively yawned, rolled their eyes, and moved on to the buffet table. One American delegate sneered that
But
Brazil’s Microbial Revolution
While Cuban and Venezuelan doctors were being ignored about mosquitoes, Brazil was building something remarkable: an entire scientific ecosystem dedicated to germ theory, almost from scratch. The catalyst? Bubonic plague arriving in the port of Santos in 1899. Nothing motivates public health investment like the
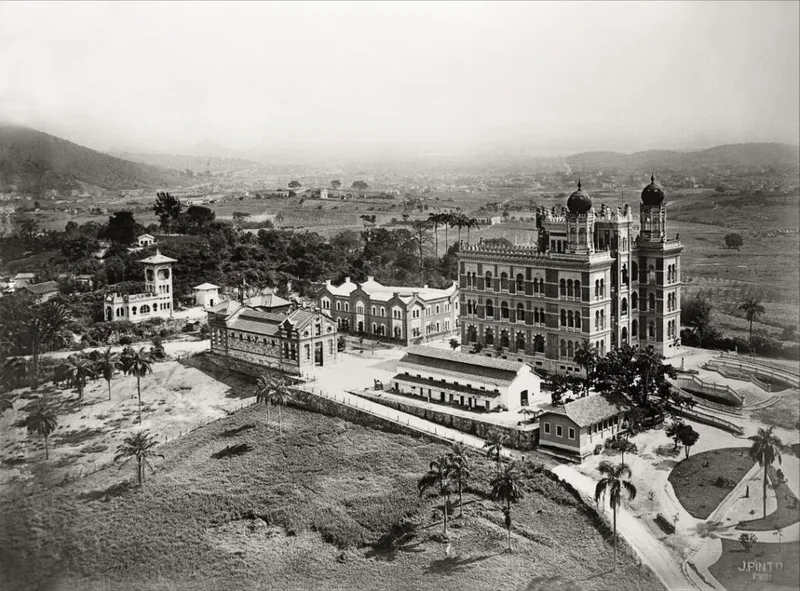
The Brazilian government, suddenly very interested in microscopic organisms, established the Federal Serum Therapy Institute on the outskirts of Rio de Janeiro. They appointed a young physician named
And deliver he did. Within months, Cruz’s team was producing effective anti-plague serum and vaccines. This was Brazil’s scientific declaration of independence—no longer importing European remedies but creating its own. Of course, Cruz wasn’t working alone. In São Paulo, a Swiss-Brazilian physician named
Together, these institutes formed a scientific triangle that would transform Brazilian medicine. But the real test would be applying this new knowledge in the real world—and that’s where things got complicated. And by “complicated,” I mean “there was literally a revolt.”
When Public Health Gets Controversial
In 1903, Brazilian President Rodrigues Alves made a decision that would either be remembered as visionary or catastrophic: he appointed 30-year-old

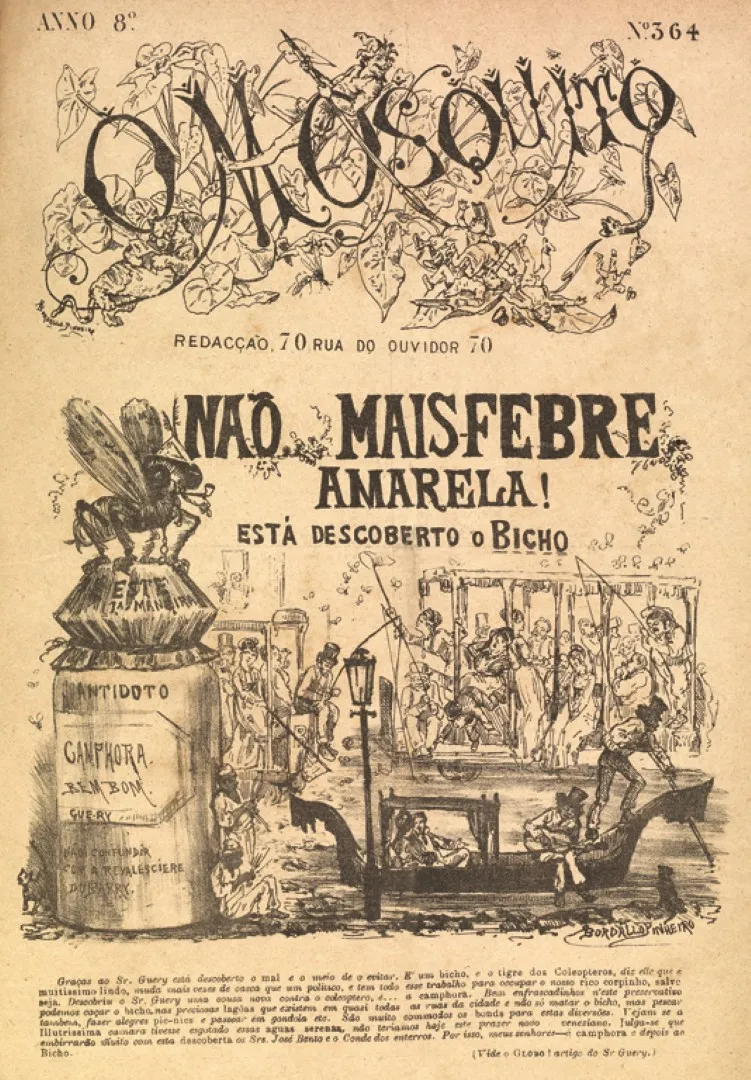
Cruz targeted three diseases with military precision: yellow fever, bubonic plague, and smallpox. His methods were… let’s call them “assertive.” For yellow fever, he deployed “mosquito brigades” to systematically destroy breeding sites throughout the city. For plague, he organised rat-catching campaigns, paying citizens by the rat. And for smallpox, he pushed through a mandatory vaccination program. Now, Cruz was fully aware of how extreme his methods appeared. His approach was uncompromising because he believed the public health crisis demanded nothing less than total commitment.
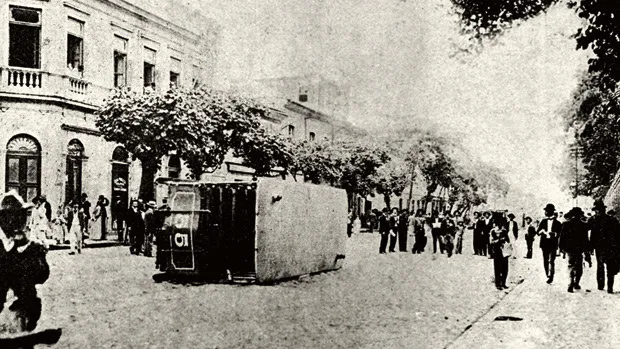
Unsurprisingly, opposition was fierce. Political cartoonists had a field day, depicting Cruz as a mad scientist wielding giant syringes like weapons. One newspaper called him a “scientific dictator” treating citizens “like laboratory rats.” The 19th-century anti-vaxxers were surprisingly creative with their rhetoric—perhaps the one area where they outperformed their modern counterparts… The situation exploded in November 1904 with the

But here’s the plot twist:
In São Paulo, physician
This scientific bravery wasn’t limited to Brazil. In Peru, medical student
“The One-Man Discovery Machine”
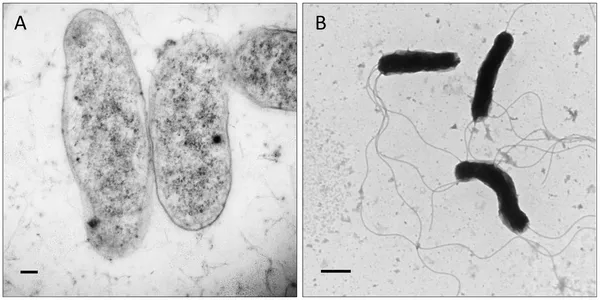
While urban centres were being transformed by militant mosquito hunters, a young Brazilian doctor named
While treating patients,

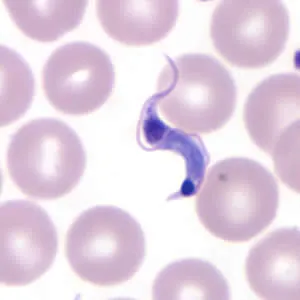
In his 1909 report to the Brazil-Medico journal, Chagas wrote with justified pride: “We believe this to be the first time that a researcher has the opportunity to study, from the beginning, the entire life cycle of a human pathogenic trypanosoma, as well as to establish experimentally the role of an arthropod in its transmission.” News of Chagas’ discovery spread through the scientific world. In 1912, he received the prestigious Schaudinn Prize for the most important discovery in parasitology. He was nominated twice for the Nobel Prize in Medicine.
But—and you knew there was going to be a “but”—despite being the only nominee in 1921, Chagas was not awarded the Nobel Prize. The committee chose to make no award that year rather than recognise the Brazilian scientist. It’s like when a teacher says “I’d rather give everyone a zero than award points for this answer from this student I don’t really like”—except instead of a classroom assignment, it was one of the most important medical discoveries of the century. Talk about academic snobbery! And this wasn’t just academically important—it revealed a hidden health crisis affecting millions of rural Latin Americans. Chagas disease still affects 6-7 million people today, particularly in poor, rural areas.
In later writings, Chagas reflected on how tropical medicine revealed social inequalities: “The great diseases that devastate humanity are the sad privilege of poor populations. Tuberculosis, leprosy, and in our country, this trypanosomiasis… are the consequences of abandonment, of the absence of prophylactic defense.” This social consciousness became a hallmark of Latin American public health—recognising that controlling disease meant addressing poverty and inequality. While European bacteriologists were focused on microbes in petri dishes, Latin American scientists were confronting the social conditions that allowed those microbes to thrive.
From Student to Teacher
By the 1910s, Latin American scientists had completed a remarkable transformation: from students of European methods to innovative practitioners and teachers in their own right. The
At the 1913 International Congress of Medicine in London, Brazilian tropical medicine was featured prominently.
Latin American scientists had moved from being recipients of European knowledge to contributors to global scientific discourse. They published in international journals, presented at conferences, and established their own scientific traditions. What made their contributions distinctive? Three things:
First, necessity drove innovation. When yellow fever is killing thousands in your city, you don’t have the luxury of academic debates—you need solutions now. This pragmatism led to bold public health interventions and self-experiments that might have been considered too risky or unconventional. Second, Latin American scientists excelled at synthesising laboratory science with field epidemiology.
By the 1920s, the flow of scientific knowledge had become bidirectional. European and North American researchers were studying Latin American methods of disease control and vector management. The “periphery” had become, in some areas, closer to the centre.
Final Thoughts: Rewriting the Microbial Map
The story of
What prevented their full recognition? Partly it was the scientific hierarchy, where discoveries made outside recognised centers faced extra scrutiny. Partly it was language barriers—publications in Portuguese or Spanish reached smaller audiences. But it was also tied to broader stereotypes about the tropics as places of disease rather than medical innovation. There’s a lot of racism that is pretty hard to ignore, too. This Eurocentric bias has consequences even today. When the Zika virus outbreak hit Brazil in 2015, it was Brazilian scientists at the
So, the next time you hear about how germ theory changed the world, remember the microbe hunters of the tropics, who not only embraced this new science but advanced it in crucial ways. I’ll leave you with a question: what other areas of history might look different if we stopped seeing the world through a Eurocentric lens? What other contributions have we overlooked? Because like those 19th-century doctors who missed the mosquitoes for the miasma, we might be missing the most interesting parts of the story. If you enjoyed this text, please consider becoming a patron and supporting my work on Patreon, it truly helps. Muito obrigada e tchau tchau!
References
Louis-Daniel Beauperthuy, Sobre la causa de la fiebre amarilla (Caracas, 1854).
Vital Brazil, A defesa contra o veneno das serpentes (São Paulo, 1911).
Daniel Alcides Carrión, Informe sobre la verruga peruana (Lima, 1885).
Carlos Chagas, Nova tripanozomiaze humana: Estudos sobre a morfolojia e o ciclo evolutivo do Schizotrypanum cruzi n. gen., n. sp., ajente etiolojico de nova entidade morbida do homem, in Memórias do Instituto Oswaldo Cruz, 1 (1909), pp. 159–218.
Oswaldo Cruz, A campanha contra a peste bubônica no Rio de Janeiro (Rio de Janeiro, 1900).
Marcos Cueto, The Value of Health: A History of the Pan American Health Organization (Washington, D.C., 2007).
Mariola Espinosa, Epidemic Invasions: Yellow Fever and the Limits of Cuban Independence, 1878–1930 (Chicago, 2009).
Carlos Finlay, El mosquito hipotéticamente considerado como agente de transmisión de la fiebre amarilla (Havana, 1881).
Gilberto Hochman, A era do saneamento: As bases da política de saúde pública no Brasil (São Paulo, 1998).
Robert Koch, Die Ätiologie der Tuberkulose (Berlin, 1882).
Simone Petraglia Kropf and Magali Romero Sá, Ciência e paixão: A trajetória de Carlos Chagas (Rio de Janeiro, 2009).
John E. Lesch, The First Miracle Drugs: How the Sulfa Drugs Transformed Medicine (Oxford, 2007).
Ilana Löwy, Vírus, mosquitos e modernidade: A febre amarela no Brasil entre ciência e política (Rio de Janeiro, 2006).
Adolfo Lutz, Contribuições ao estudo das febres tropicais (São Paulo, 1892).
Louis Pasteur, Mémoire sur la fermentation appelée lactique, in Annales de Chimie et de Physique, 52 (1858), pp. 404–418.
Walter Reed, The Etiology of Yellow Fever: A Preliminary Note, in Philadelphia Medical Journal, 6 (1900), pp. 790–796.
Emílio Ribas, A febre amarella e os mosquitos (São Paulo, 1903).
Nancy Leys Stepan, Eradication: Ridding the World of Diseases Forever? (Ithaca, 2011).