The Tiffany Problem: 10 'Modern' Things That Are Way Older Than You Think
From ancient Roman fast food to medieval almond milk—ten things that feel modern but have been around for centuries.

Medieval True Crime: When a Corpse Solved Its Own Murder
In 1503 Switzerland, Hans Spiess was forced to touch his wife's corpse—if it bled, he was guilty. Discover the medieval bier ordeal trial.

The Censored Witches' Flying Potion (That Promised a "Lover")
Uncover Della Porta's infamous 16th-century witches' ointment recipe—hallucinogenic herbs, erotic visions, and Inquisition censorship.

Fake Virginity: The Painful Renaissance ‘Cures’ They Sold Women
Discover dangerous Renaissance recipes for faking virginity—blistering pills, leeches, and lead paint sold to women facing ruin without wedding-night blood.

How Water Cures Revolutionised Medicine in the 16th Century
Discover Renaissance spa culture—from fertility baths in Naples to Leonardo Fioravanti's water cures that challenged traditional medicine.

How Latin America Shaped Germ Theory
Discover how Latin American scientists pioneered mosquito transmission theory and disease eradication—decades before European recognition.

Hypocras: The Spiced Wine Medieval Doctors Prescribed as Medicine
Hypocras was served at royal banquets and prescribed by physicians. The history of the spiced wine that blurred the line between medicine and pleasure.
The Yellow Wallpaper: The Medical History Behind Charlotte Perkins Gilman's Story
Charlotte Perkins Gilman wrote The Yellow Wallpaper as a response to the rest cure. The real medical context behind one of literature's most unsettling stories.

Urine Tests in the Renaissance: How Doctors Diagnosed Pregnancy and Fertility
Centuries before modern pregnancy tests, physicians examined urine colour, sediment, and even mixed it with wine. The strange science of Renaissance uroscopy.
Birth Trays in Renaissance Italy and Motherhood
After the Black Death devastated Italy, ornate birth trays celebrated motherhood and encouraged childbirth—discover their art, ritual, and symbolism.
Dracula and the History of Blood Transfusions: Science, Sex, and Victorian Anxiety
Bram Stoker wrote Dracula as blood transfusion was becoming real medicine. How the novel reflects Victorian fears about science, sexuality, and women's bodies.
17th Century "Intuitive Eating": Paracelsus and Digestion
Discover how Paracelsian medicine revolutionized 17th-century diet advice, empowering people to trust their bodies over doctors' rules.
What were the "Non-Naturals"?
Learn about the six non-naturals—air, food, sleep, exercise, evacuation, and emotions—that shaped preventive medicine for centuries.

Alchemy in the Renaissance: The Mysterious Isabella Cortese
Uncover Isabella Cortese, the enigmatic 16th-century alchemist whose bestselling book challenged tradition and championed women's knowledge.

Eaglestones: Historical Amulets for Childbirth
Discover eaglestones—ancient 'pregnant' geodes believed to protect women during childbirth, from Greek antiquity to 19th-century England.
Caterina Sforza's Experiments: Alchemy, Medicine, and Power in Renaissance Italy
Caterina Sforza left behind over 450 recipes for medicines, cosmetics, and poisons. What her alchemical notebook reveals about Renaissance women and power.
Green Sickness: A Historical Look at the 'Disease of Virgins'
Explore the mysterious disease of virgins that shaped medical control over young women from the 1550s to 1920s through marriage and motherhood.

Golden Locks: Hair Care in the Renaissance Era
Discover Renaissance hair care—from dove droppings for hair loss to sun-bleaching on Venetian rooftops for that coveted golden blonde.
Paracelsus: The Renaissance Physician Who Set Fire to Medical Tradition
He publicly burned Galen, dosed patients with mercury, and got exiled from Basel. The life and legacy of early modern medicine's most controversial figure.

Fioravanti: Pioneering Surgeon-Alchemist of the Renaissance
Leonardo Fioravanti was called a Charlatan, a Poisoner, a Reformer, a Prophet, a Miracle-Worker, a Saviour, an Alchemist, and a Fraud.

The Medicine behind food – from starters to desserts
Discover why we eat soup first and cheese last—the humoral theory and Renaissance medicine shaped our modern meal structure.
Frankincense and Myrrh: From Ancient Medicine to the Nativity Story
Frankincense treated wounds and plague. Myrrh eased childbirth pain. Long before the Magi, these resins were among the ancient world's most valued medicines.

Little Red Riding Hood and the Invisibility of Older Women
In early versions, Little Red Riding Hood ate her grandmother's flesh and escaped the wolf—explore menopause, aging, and female wisdom.
The 'Queen of Hysterics' and 19th-Century Theatrical Hysteria
Meet Blanche Wittmann, the 'queen of hysterics' at Charcot's Salpêtrière Hospital, where medical demonstrations became theatrical spectacles.

What is the 'Doctrine of Signatures'?
Discover how Renaissance physicians believed plants revealed their healing powers through shape, color, and resemblance to body parts.
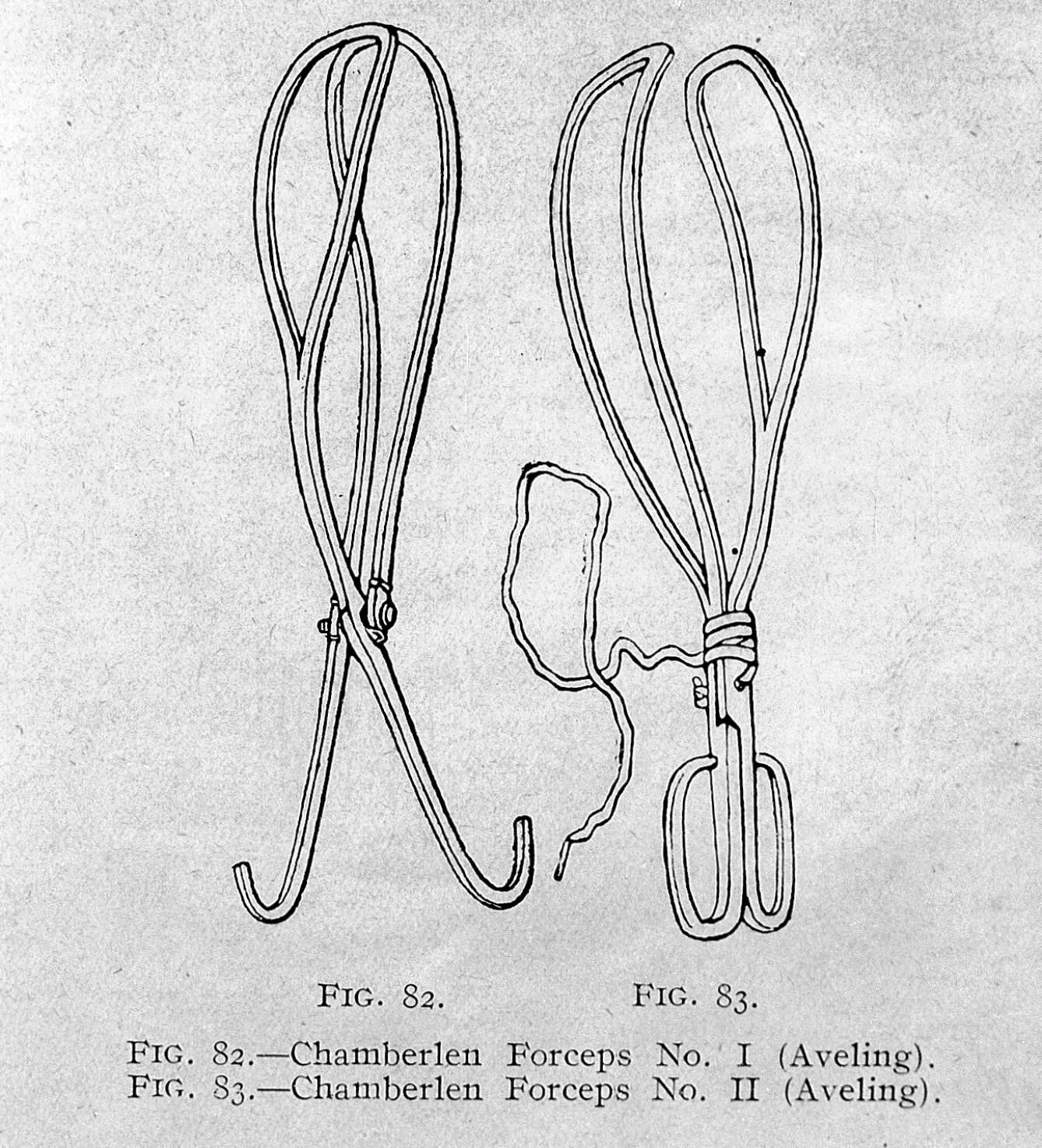
A Grip on the History of Forceps in Medicine
Discover how the Chamberlen family's secret obstetrical forceps revolutionized childbirth and transformed midwifery into modern obstetrics.

What is the ‘Wandering Womb’?
Discover the ancient Greek theory of the 'wandering womb'—an animal inside an animal, moving through the body in search of moisture.

Wet Nurses in Early Modern Europe: The History of Breastfeeding and Motherhood
Most wealthy mothers didn't breastfeed their own children. The history of wet nursing, and why it sparked fierce moral debate for centuries.

Why Did People Try to Induce Menstruation in the Past?
Discover 16th-century recipes to 'restore' menstruation—from roasted apples with nutmeg to herbal remedies that blurred the line with abortion.

The Surprising History of Abandoned Children
From Hansel and Gretel to foundling hospitals—explore the complex history of child abandonment and why 'unnatural mothers' weren't always villains.

Giving Birth in 17th-century England: A Tentative List
From groaning cakes to birthing stools—discover how 17th-century English families prepared for childbirth before hospitals and modern medicine.
Green Sickness and Virginity
Discover green sickness, the mysterious ailment that affected young women from the 1550s to 1920s—diagnosed by paleness, fainting, and virginity.
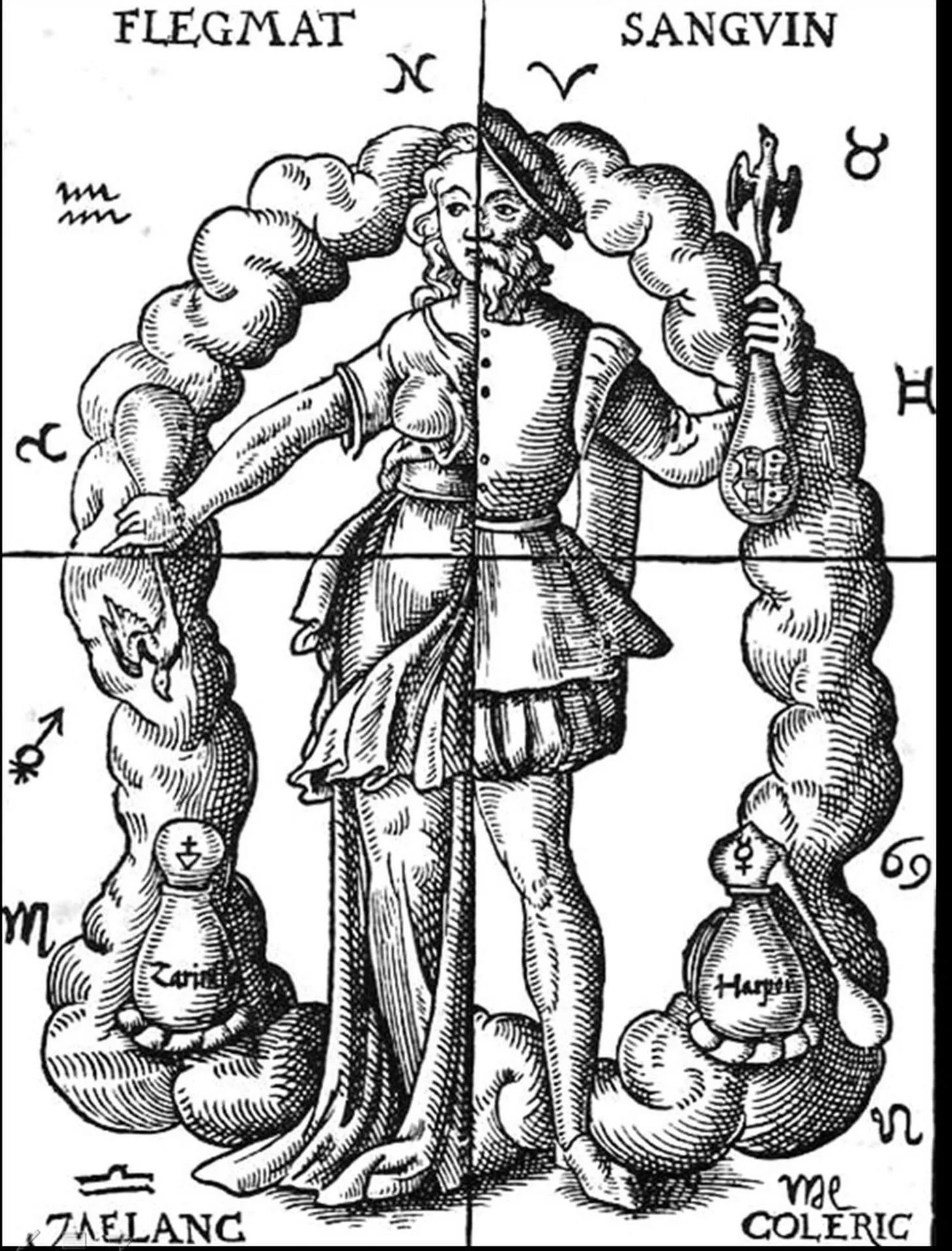
Humoral Theory: How the Four Humours Shaped Medicine for 2,000 Years
Blood, phlegm, yellow bile, and black bile — the four humours formed the foundation of Western medicine from ancient Greece to the 18th century.
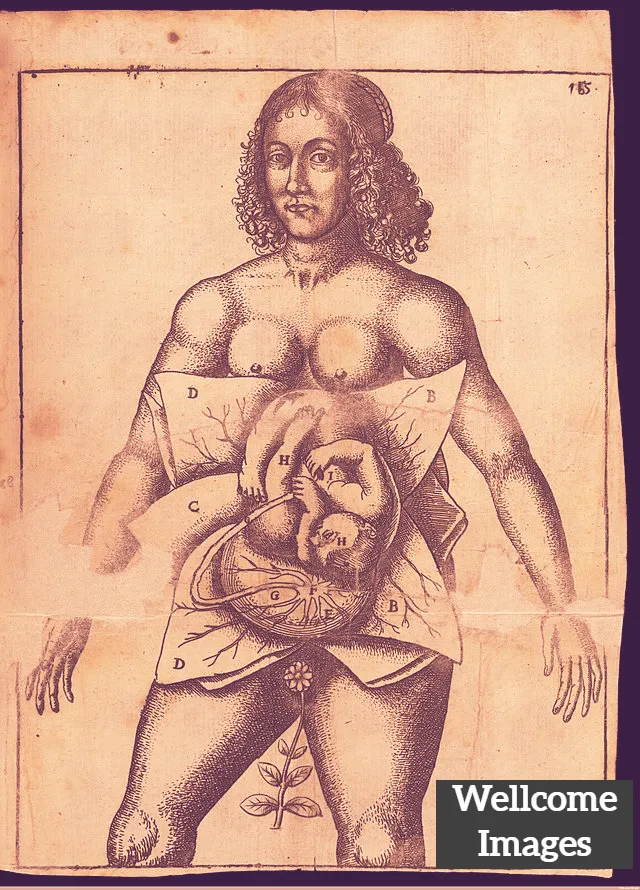
What are Secrets of Women?
Discover 'secrets of women'—early modern medical recipes for conception, menstruation, and childbirth, hidden in the mysterious feminine body.
The Tiffany Problem: 10 'Modern' Things That Are Way Older Than You Think
From ancient Roman fast food to medieval almond milk—ten things that feel modern but have been around for centuries.
Medieval True Crime: When a Corpse Solved Its Own Murder
In 1503 Switzerland, Hans Spiess was forced to touch his wife's corpse—if it bled, he was guilty. Discover the medieval bier ordeal trial.
The Censored Witches' Flying Potion (That Promised a "Lover")
Uncover Della Porta's infamous 16th-century witches' ointment recipe—hallucinogenic herbs, erotic visions, and Inquisition censorship.
Fake Virginity: The Painful Renaissance ‘Cures’ They Sold Women
Discover dangerous Renaissance recipes for faking virginity—blistering pills, leeches, and lead paint sold to women facing ruin without wedding-night blood.
How Water Cures Revolutionised Medicine in the 16th Century
Discover Renaissance spa culture—from fertility baths in Naples to Leonardo Fioravanti's water cures that challenged traditional medicine.
How Latin America Shaped Germ Theory
Discover how Latin American scientists pioneered mosquito transmission theory and disease eradication—decades before European recognition.
Hypocras: The Spiced Wine Medieval Doctors Prescribed as Medicine
Hypocras was served at royal banquets and prescribed by physicians. The history of the spiced wine that blurred the line between medicine and pleasure.
The Yellow Wallpaper: The Medical History Behind Charlotte Perkins Gilman's Story
Charlotte Perkins Gilman wrote The Yellow Wallpaper as a response to the rest cure. The real medical context behind one of literature's most unsettling stories.
Urine Tests in the Renaissance: How Doctors Diagnosed Pregnancy and Fertility
Centuries before modern pregnancy tests, physicians examined urine colour, sediment, and even mixed it with wine. The strange science of Renaissance uroscopy.
Birth Trays in Renaissance Italy and Motherhood
After the Black Death devastated Italy, ornate birth trays celebrated motherhood and encouraged childbirth—discover their art, ritual, and symbolism.
Dracula and the History of Blood Transfusions: Science, Sex, and Victorian Anxiety
Bram Stoker wrote Dracula as blood transfusion was becoming real medicine. How the novel reflects Victorian fears about science, sexuality, and women's bodies.
17th Century "Intuitive Eating": Paracelsus and Digestion
Discover how Paracelsian medicine revolutionized 17th-century diet advice, empowering people to trust their bodies over doctors' rules.
What were the "Non-Naturals"?
Learn about the six non-naturals—air, food, sleep, exercise, evacuation, and emotions—that shaped preventive medicine for centuries.
Alchemy in the Renaissance: The Mysterious Isabella Cortese
Uncover Isabella Cortese, the enigmatic 16th-century alchemist whose bestselling book challenged tradition and championed women's knowledge.
Eaglestones: Historical Amulets for Childbirth
Discover eaglestones—ancient 'pregnant' geodes believed to protect women during childbirth, from Greek antiquity to 19th-century England.
Caterina Sforza's Experiments: Alchemy, Medicine, and Power in Renaissance Italy
Caterina Sforza left behind over 450 recipes for medicines, cosmetics, and poisons. What her alchemical notebook reveals about Renaissance women and power.
Green Sickness: A Historical Look at the 'Disease of Virgins'
Explore the mysterious disease of virgins that shaped medical control over young women from the 1550s to 1920s through marriage and motherhood.
Golden Locks: Hair Care in the Renaissance Era
Discover Renaissance hair care—from dove droppings for hair loss to sun-bleaching on Venetian rooftops for that coveted golden blonde.
Paracelsus: The Renaissance Physician Who Set Fire to Medical Tradition
He publicly burned Galen, dosed patients with mercury, and got exiled from Basel. The life and legacy of early modern medicine's most controversial figure.
Fioravanti: Pioneering Surgeon-Alchemist of the Renaissance
Leonardo Fioravanti was called a Charlatan, a Poisoner, a Reformer, a Prophet, a Miracle-Worker, a Saviour, an Alchemist, and a Fraud.
The Medicine behind food – from starters to desserts
Discover why we eat soup first and cheese last—the humoral theory and Renaissance medicine shaped our modern meal structure.
Frankincense and Myrrh: From Ancient Medicine to the Nativity Story
Frankincense treated wounds and plague. Myrrh eased childbirth pain. Long before the Magi, these resins were among the ancient world's most valued medicines.
Little Red Riding Hood and the Invisibility of Older Women
In early versions, Little Red Riding Hood ate her grandmother's flesh and escaped the wolf—explore menopause, aging, and female wisdom.
The 'Queen of Hysterics' and 19th-Century Theatrical Hysteria
Meet Blanche Wittmann, the 'queen of hysterics' at Charcot's Salpêtrière Hospital, where medical demonstrations became theatrical spectacles.
What is the 'Doctrine of Signatures'?
Discover how Renaissance physicians believed plants revealed their healing powers through shape, color, and resemblance to body parts.
A Grip on the History of Forceps in Medicine
Discover how the Chamberlen family's secret obstetrical forceps revolutionized childbirth and transformed midwifery into modern obstetrics.
What is the ‘Wandering Womb’?
Discover the ancient Greek theory of the 'wandering womb'—an animal inside an animal, moving through the body in search of moisture.
Wet Nurses in Early Modern Europe: The History of Breastfeeding and Motherhood
Most wealthy mothers didn't breastfeed their own children. The history of wet nursing, and why it sparked fierce moral debate for centuries.
Why Did People Try to Induce Menstruation in the Past?
Discover 16th-century recipes to 'restore' menstruation—from roasted apples with nutmeg to herbal remedies that blurred the line with abortion.
The Surprising History of Abandoned Children
From Hansel and Gretel to foundling hospitals—explore the complex history of child abandonment and why 'unnatural mothers' weren't always villains.
Giving Birth in 17th-century England: A Tentative List
From groaning cakes to birthing stools—discover how 17th-century English families prepared for childbirth before hospitals and modern medicine.
Green Sickness and Virginity
Discover green sickness, the mysterious ailment that affected young women from the 1550s to 1920s—diagnosed by paleness, fainting, and virginity.
Humoral Theory: How the Four Humours Shaped Medicine for 2,000 Years
Blood, phlegm, yellow bile, and black bile — the four humours formed the foundation of Western medicine from ancient Greece to the 18th century.
What are Secrets of Women?
Discover 'secrets of women'—early modern medical recipes for conception, menstruation, and childbirth, hidden in the mysterious feminine body.