Green Sickness: A Historical Look at the 'Disease of Virgins'
Explore the mysterious disease of virgins that shaped medical control over young women from the 1550s to 1920s through marriage and motherhood.
What Made a 17th-Century Midwife Good at Her Job?
Percivall Willughby despised 17th-century midwives—but were his brutal accusations true? Explore what really made a good midwife in 1600s England.
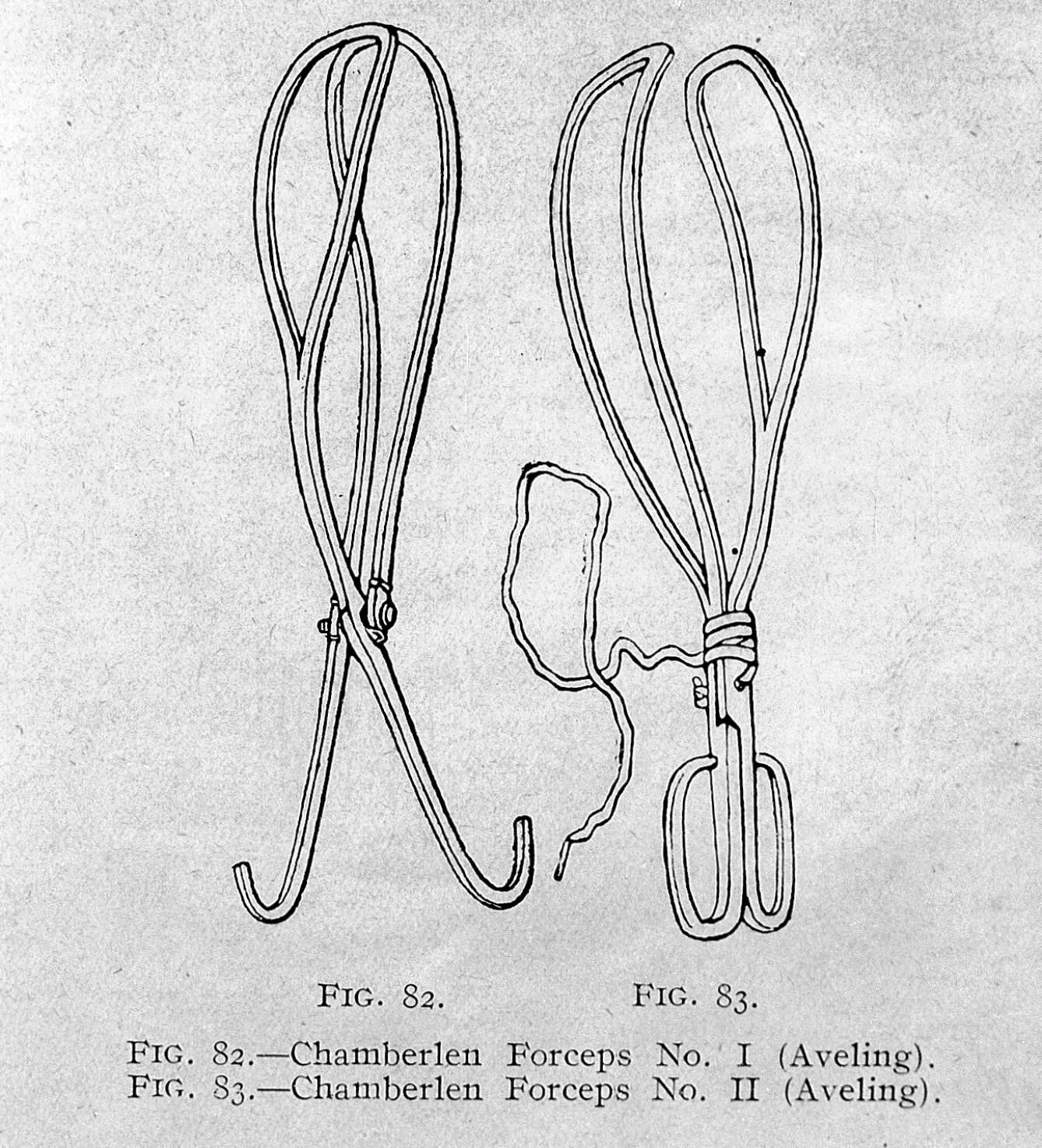
A Grip on the History of Forceps in Medicine
Discover how the Chamberlen family's secret obstetrical forceps revolutionized childbirth and transformed midwifery into modern obstetrics.

Giving Birth in 17th-century England: A Tentative List
From groaning cakes to birthing stools—discover how 17th-century English families prepared for childbirth before hospitals and modern medicine.

‘Let Nature Take its Course’: In Defence of ‘Gentle’ Midwifery
Meet Louise Bourgeois, the 16th-century French royal midwife who championed calm, gentle childbirth—centuries before modern birthing philosophy.
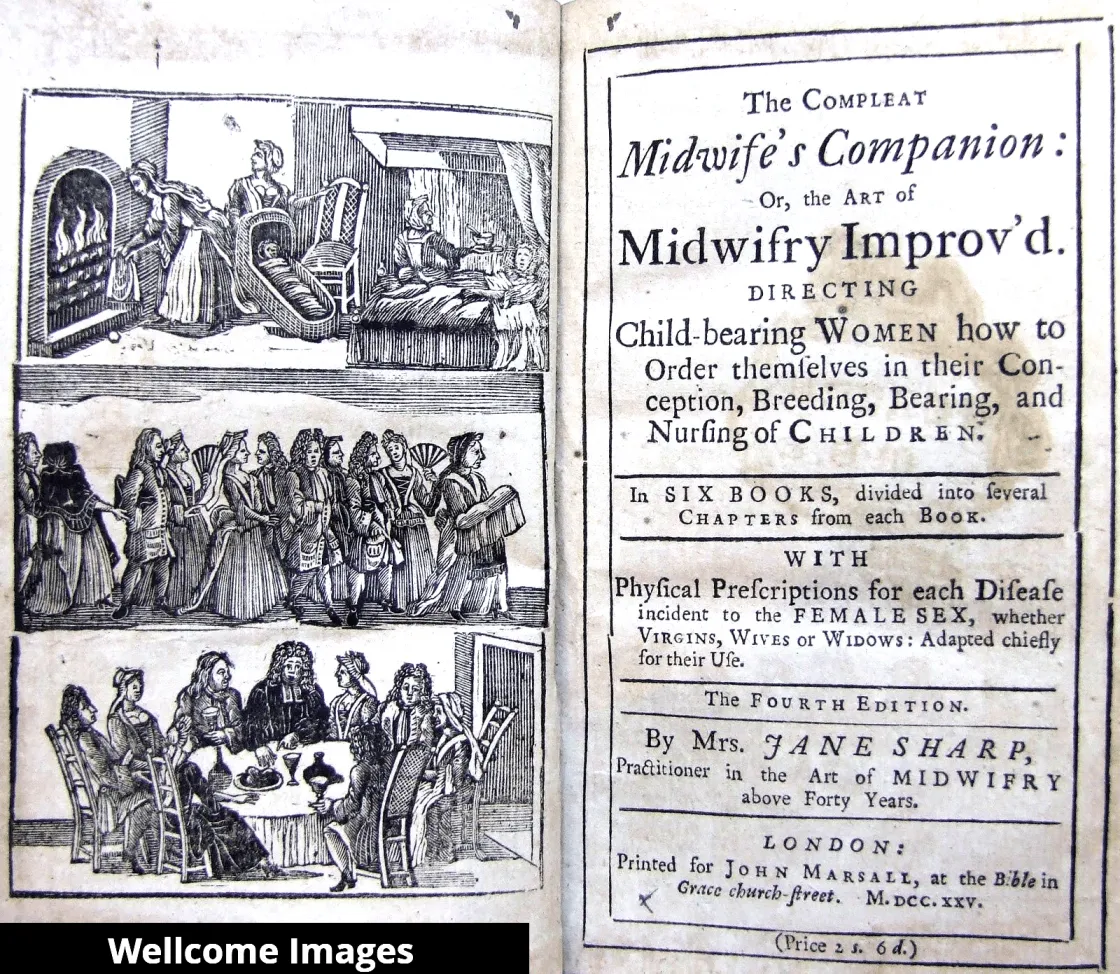
'…but the Art of Midwifry chiefly concern us'!
Jane Sharp's 1671 midwifery manual celebrated midwives as essential—yet centuries later, they still fight for respect and recognition.
Green Sickness: A Historical Look at the 'Disease of Virgins'
Explore the mysterious disease of virgins that shaped medical control over young women from the 1550s to 1920s through marriage and motherhood.
What Made a 17th-Century Midwife Good at Her Job?
Percivall Willughby despised 17th-century midwives—but were his brutal accusations true? Explore what really made a good midwife in 1600s England.
A Grip on the History of Forceps in Medicine
Discover how the Chamberlen family's secret obstetrical forceps revolutionized childbirth and transformed midwifery into modern obstetrics.
Giving Birth in 17th-century England: A Tentative List
From groaning cakes to birthing stools—discover how 17th-century English families prepared for childbirth before hospitals and modern medicine.
‘Let Nature Take its Course’: In Defence of ‘Gentle’ Midwifery
Meet Louise Bourgeois, the 16th-century French royal midwife who championed calm, gentle childbirth—centuries before modern birthing philosophy.
'…but the Art of Midwifry chiefly concern us'!
Jane Sharp's 1671 midwifery manual celebrated midwives as essential—yet centuries later, they still fight for respect and recognition.