The Midwife’s Ghost: A Murder Ballad from 1680
Discover the haunting 1680 ballad of a murdered midwife's ghost—sensationalized news set to music, recorded by Samuel Pepys himself.
Birth Trays in Renaissance Italy and Motherhood
After the Black Death devastated Italy, ornate birth trays celebrated motherhood and encouraged childbirth—discover their art, ritual, and symbolism.

Eaglestones: Historical Amulets for Childbirth
Discover eaglestones—ancient 'pregnant' geodes believed to protect women during childbirth, from Greek antiquity to 19th-century England.
What Made a 17th-Century Midwife Good at Her Job?
Percivall Willughby despised 17th-century midwives—but were his brutal accusations true? Explore what really made a good midwife in 1600s England.

Maternal Mortality and a Mother's Last Letter
Elizabeth Joceline's heartbreaking 1622 letter to her unborn child—a testament to maternal love and the perils of early modern childbirth.
A Grip on the History of Forceps in Medicine
Discover how the Chamberlen family's secret obstetrical forceps revolutionized childbirth and transformed midwifery into modern obstetrics.

The Surprising History of Abandoned Children
From Hansel and Gretel to foundling hospitals—explore the complex history of child abandonment and why 'unnatural mothers' weren't always villains.

Giving Birth in 17th-century England: A Tentative List
From groaning cakes to birthing stools—discover how 17th-century English families prepared for childbirth before hospitals and modern medicine.

‘Let Nature Take its Course’: In Defence of ‘Gentle’ Midwifery
Meet Louise Bourgeois, the 16th-century French royal midwife who championed calm, gentle childbirth—centuries before modern birthing philosophy.

'Before she was in labour, she gave birth'
Explore how medieval theology imagined Mary's miraculous, painless childbirth—skipping labor entirely to preserve her virginal purity.
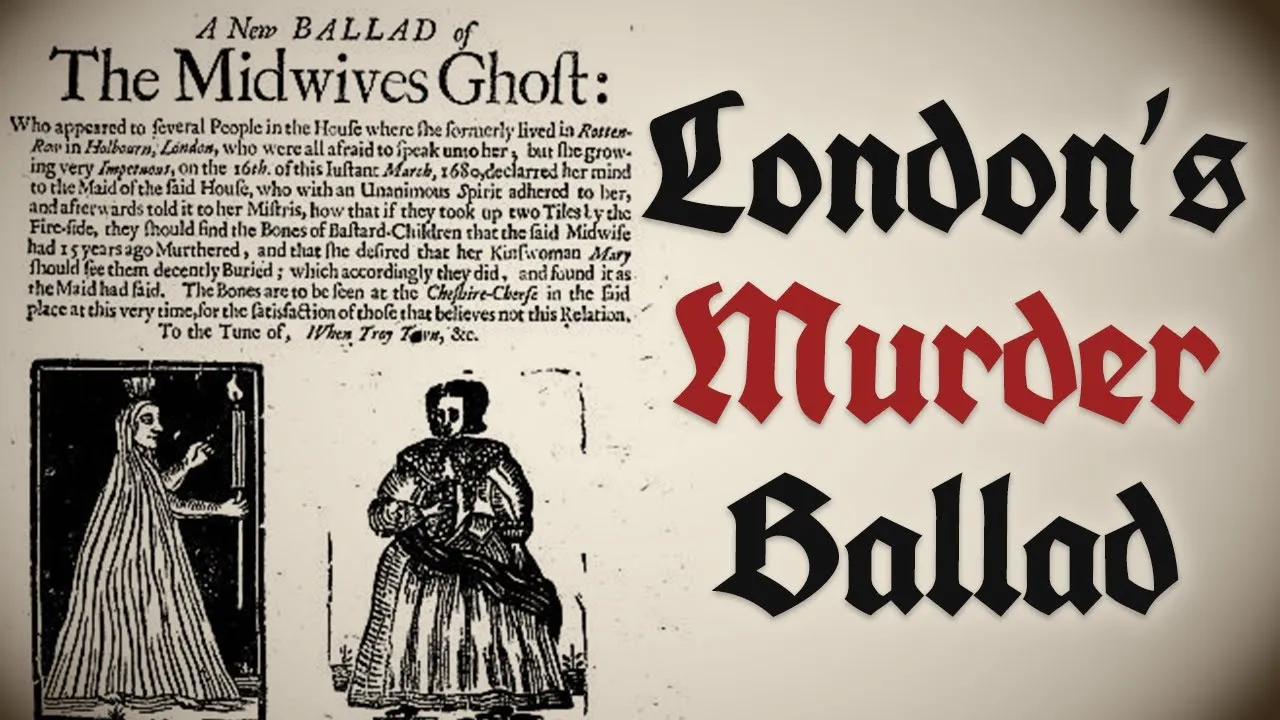
The Midwife’s Ghost: A Murder Ballad from 1680
Discover the haunting 1680 ballad of a murdered midwife's ghost—sensationalized news set to music, recorded by Samuel Pepys himself.
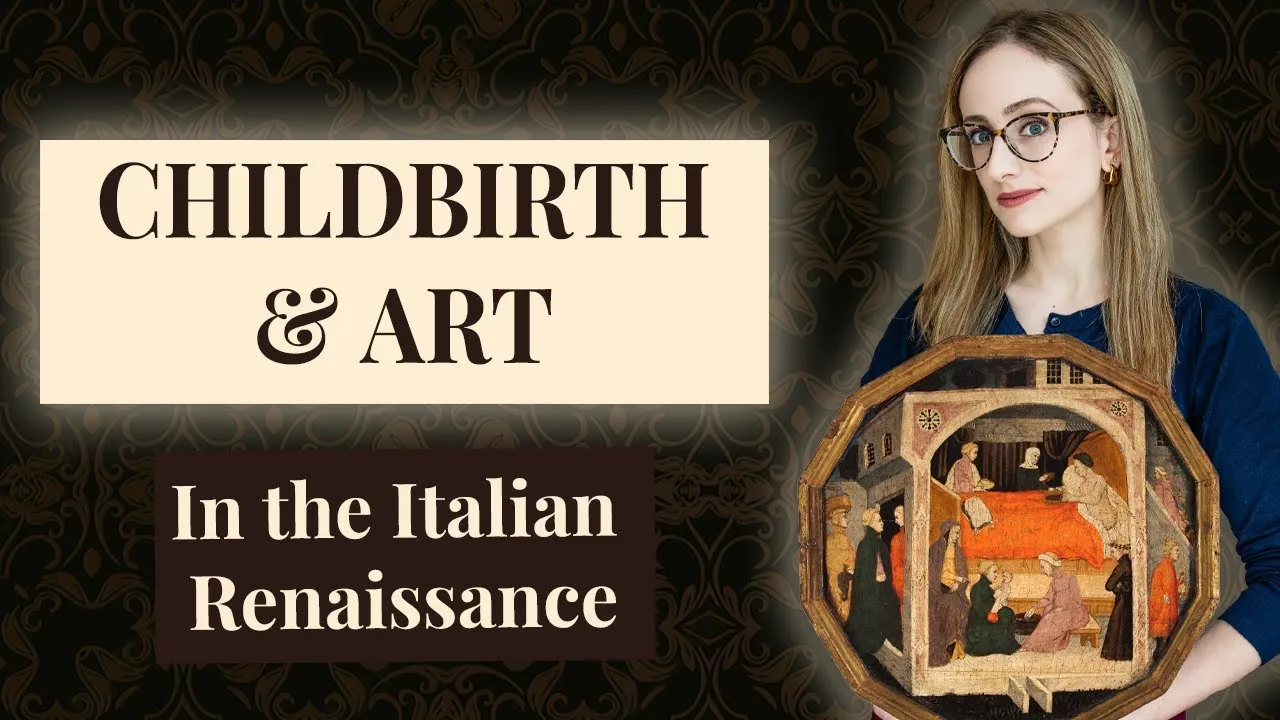
Birth Trays in Renaissance Italy and Motherhood
After the Black Death devastated Italy, ornate birth trays celebrated motherhood and encouraged childbirth—discover their art, ritual, and symbolism.
Eaglestones: Historical Amulets for Childbirth
Discover eaglestones—ancient 'pregnant' geodes believed to protect women during childbirth, from Greek antiquity to 19th-century England.
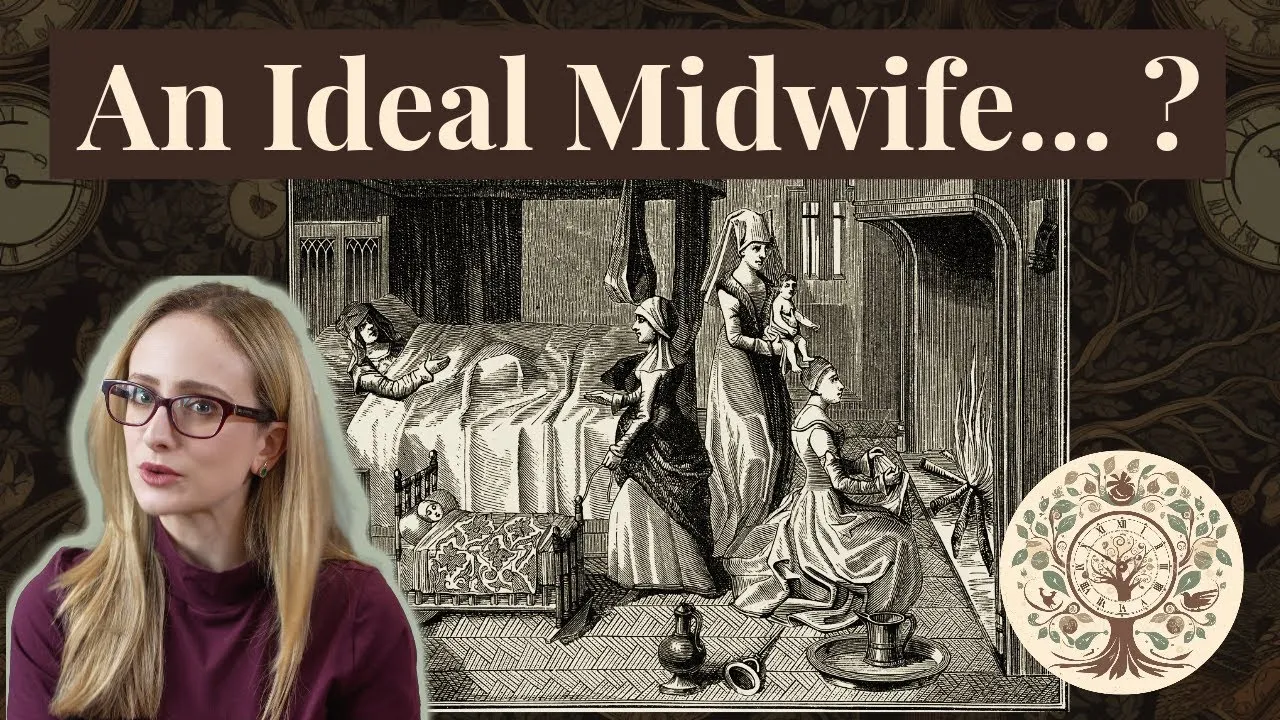
What Made a 17th-Century Midwife Good at Her Job?
Percivall Willughby despised 17th-century midwives—but were his brutal accusations true? Explore what really made a good midwife in 1600s England.
Maternal Mortality and a Mother's Last Letter
Elizabeth Joceline's heartbreaking 1622 letter to her unborn child—a testament to maternal love and the perils of early modern childbirth.
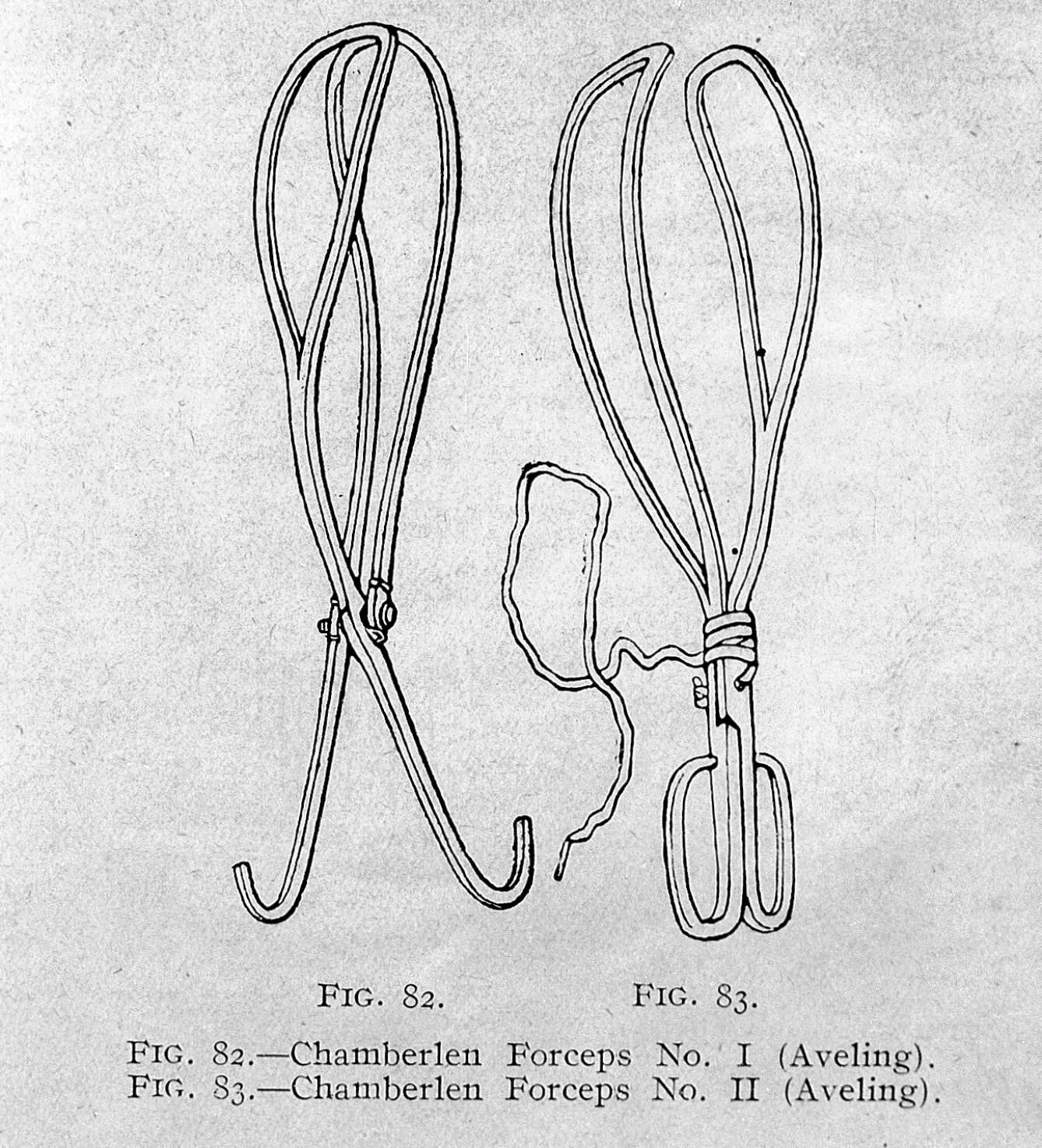
A Grip on the History of Forceps in Medicine
Discover how the Chamberlen family's secret obstetrical forceps revolutionized childbirth and transformed midwifery into modern obstetrics.
The Surprising History of Abandoned Children
From Hansel and Gretel to foundling hospitals—explore the complex history of child abandonment and why 'unnatural mothers' weren't always villains.
Giving Birth in 17th-century England: A Tentative List
From groaning cakes to birthing stools—discover how 17th-century English families prepared for childbirth before hospitals and modern medicine.
‘Let Nature Take its Course’: In Defence of ‘Gentle’ Midwifery
Meet Louise Bourgeois, the 16th-century French royal midwife who championed calm, gentle childbirth—centuries before modern birthing philosophy.
'Before she was in labour, she gave birth'
Explore how medieval theology imagined Mary's miraculous, painless childbirth—skipping labor entirely to preserve her virginal purity.